Stricture
Urology Surgery And Results
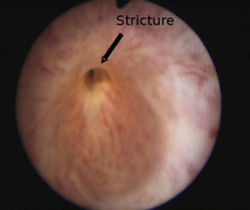
Urethral Stricture
Urethra is the pipe-shaped organ in the penis from where we pass urine. Blockage to this passage causes symptoms where a patient has poor urine flow. This is called a stricture.
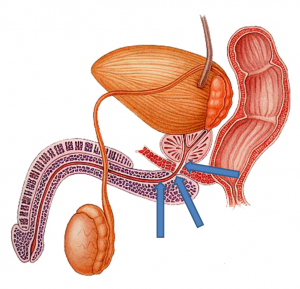
Anatomy
Urethra is divided in two parts :
- Anterior Urethra
- Posterior Urethra.
Anterior Urethra is further divided in to 2 parts
- Penile Urethra: Lies in the penis
- Bulbar Urethra: It is located behind and below the scrotum
Posterior Urethra consists of
- Membranous Urethra—It is the spring, which controls urine and avoids leakage
- Prostatic Urethra.
Etiology
Anterior Urethral strictures usually occurs due to:
- Instrumentation
- After Foleys catheter
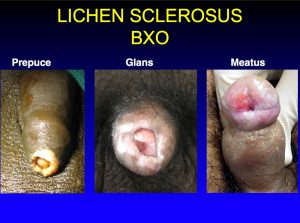
- Lichen Sclerosus (Skin Disease where skin color is white)
- Sexually transmitted infections
- Trauma
- Idiopathic (Cause not known)
- This stricture can occur in Bulbar Urethra or Penile Urethra or Pan urethra (Whole Urethra)
Posterior Urethral Stricture Occurs due to:
- Trauma
- Called as PFUDD (Pelvic Fracture Urethral Distraction Defect)
- or PFUI ( Pelvic Fracture Urethral Injury)
Symptoms
- Patients have poor flow
- Burning of urine
- Straining to pass urine
- Bleeding at end of Urine
- Feeling of incomplete evacuation
Rarely if neglected , then patients develops Kidney failure as urine gets stagnated in bladder and kidneys.
Investigations
Clinical Examination
Patient is examined thoroughly including detailed genital examination. Causes of stricture such as lichen sclerosus is checked. In this skin disease there are white spots on the glans which is the tip of penis.
Uroflowmetery
Patient is asked to drink water and inform us when he wants to pass urine. He is then requested to urinate in a special toilet which is connected to a computer. Normal urine flow is smooth and bell-shaped curved. Speed to urine is about 15-20 ml/sec. In stricture this flow decreases

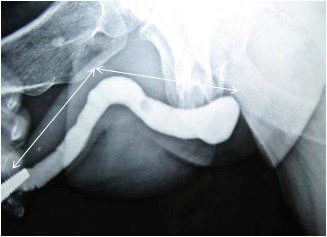
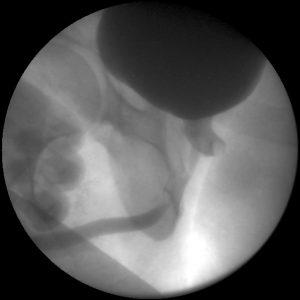
Urethrogram
This is performed in the OT where there are sterile precautions. Medicine called as contract is put in the urine passage gently.
The photograph of the urethra is taken on an x-ray while putting the contrast and while passing urine. This tells us the exact location of stricture.
This is a painless procedure and most informative.
Sonourethrography
Sometimes we send patients to perform Ultrasonography of the urethra. It tells us about the presence of fibrous scarred tissue labeled as spongiofibrosis in urethra. It also tells us about the bladder status and kidney status and the residual urine.
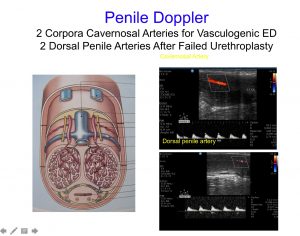
Penile Doppler
This test is performed in patients who have urethral injury due to pelvic bone fracture. Patients are referred to as the compitent radiologist. A small injection is given in the Penis to look for erection and then velocity is measured in the penile vessels.
This test takes about 30 minutes.
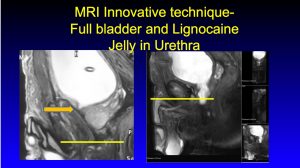
MRI
- In patients with Pelvic fracture Urethral injury MRI scan may be required to look for bladder neck status and the gap of urethral stricture.
Treatment of Anterior Urethral Stricture
Penile Urethra Stricture
Penile stricture should not be treated with DVIU (Endoscopic cuts) or repeated dilatations. Urethroplasty offers the best cure for Penile strictures. For treatment management, we divide penile strictures into 2 categories –Failed hypospadias and Others.
Failed Hypospadias:
Patients with multiple failed hypospadias repairs can develop penile strictures, fistula, and chordee. We have invented a new technique of Penile urethroplasty which has been Published and widely accepted all over the world. We make the urethra hypospadias in the first stage and then 6 months later we insert a buccal graft and close the urethra same time.
This is far better as compared to a staged buccal graft where there is a chance of graft contracting.
For all other strictures we perform the Kulkarni Approach for Urethroplasty.
Who wants an incision on Penis? No one likes it
- In Kulkarni approach through a small incision below the scrotum, the urethra is dissected.
- No incision is made on Penis unless required
- The urethra is opened and stricture identified.
- Adequate sized buccal mucosa from inside cheek is removed under full anesthesia.
- It is used to patch the wall of urethra.
- 14 Size urine Foleys catheter is kept.
- The surgical area is closed and dressing done.
Bulbar Urethra stricture
The principle remains the same as in penile urethral stricture surgery. Two types of surgery are possible
- Dorsal Onlay: Where the patch is applied on the back wall of the urethra
- Ventral Onlay: Where the patch is applied on the front wall of the urethra.
Choice of Surgery depends on factors like location of stricture, type of stricture and surgeons preference.
14 Size Urine Foley’s catheter is kept and dressing done. Foleys catheter is removed after 4 weeks.
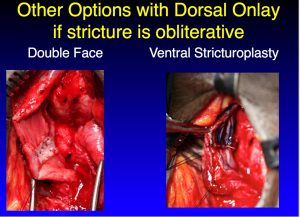
Double Face Urethroplasty
In Obliterative strictures where the urine passage is very narrow,we occasionally have to make both the walls of the urethra. Dorsal onlay with Ventral inlay or ventral onlay with dorsal inlay.This is called as Double face urethroplasty
Panurethral Stricture
Dr. Kulkarni was instrumental in pioneering the management of Panurethral stricture. It is a complex disease involving the whole urethra
Earlier the surgeons used to open up urethra along the wall and make a urine passage near the anal canal called urethrostomy. The patient would then require 2 or 3 stage surgeries after 6 months. Dr. Kulkarni described a technique where he does a single stage repair of the whole urethra without making any cut on the penis. Thus a full-length panurethral stricture is treated with a small incision. In our center, we do the highest number of panurethral stricture repairs in the world. Today world over this technique is appreciated and practiced widely.
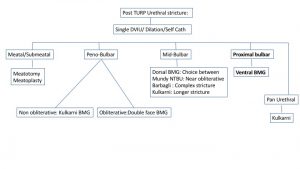
POST TURP /HOLEP/THULIUM Prostate Surgery Strictures:
Instrumentation can cause urethral strctures. We commonly get a referral for such strictures.
Usually, the stricture is in the proximal bulbar urethra and occasionally can be an entire length. Patients are on multiple dilatations and DVIU due to fear of Incontinence. We perform Ventral Onlay Bucal graft Urethroplasty in such patients with almost “0” risk of incontinence. We have recently published extensively on the above topic and have demonstrated this surgery in Live workshops.
Pelvic Fracture Urethral Distraction defect (PFUDD)
Pelvic Fracture Urethral injury (PFUI)
This is an injury to the urethra where due to fracture in the pelvic bone the 2 ends of urethra get cut and go away from each other. This is a complex condition. It may be associated with the rectal injury.
Best available treatment includes doing Supra Pubic Catheter and surgery after 3 months.Dr. Kulkarni specializes in the management of such urethral injury.
His center performs one of the largest numbers of this surgery today.
He gets a referral from all over the world. The surgery takes about 1 1/2 to 2 hours. It consists of joining the 1 cut ends together through a small incision in the perineum. So far we have performed more than 1400 Surgeries for Pelvic Fracture Urethral distraction defects.
Results
- Penile Urethra: Our Success rate: 84 %
- Bulbar Urethra: Our Success rate:86% for dorsal and ventral onlay urethroplasty
- Panurethral Stricture: Our Success rate:” Kulkarni Technique ” 80 %
- Posterior Urethra:Our Success rate:86% for primary and redo urethroplasty
Hypospadias
This is a congenital condition seen in children.
The meatus (place on penis where urine comes out) is located at an abnormal position. It is located much below than ideal. This condition requires a delicate surgical correction. Our center specializes in the management of hypospadias. We get more than 100 failed hypospadias patients every year who have been operated all across the world. We have published our novel technique of failed hypospadias surgery which has received more than 1000 views all across the globe.
It can be :
- Glandular
- Coronal
- Penile Shaft
- Peno Scrotal
- Perineal
Lots of children are having problems with urethral strictures in penile region due to inappropriate hypospadias surgery.
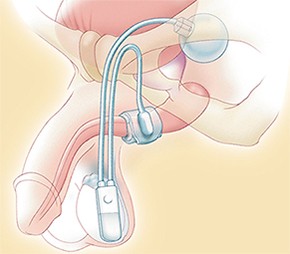
Artificial Sphincter
Incontinence means leakage of urine. This is a growing problem. It can be functional or related to surgery. Radical Prostatectomy, Pelvic Fractures, Radiation, TURP …. May cause urinary incontinence. It is due to damage to the urinary sphincter. Today it is possible for appropriately selected patients to be almost completely continent with Implantation of artificial sphincter.
This surgery is life-changing for patients who have been suffering from Urinary Incontinence.
The surgery involves making a small incision in the perineum. A cuff is inserted around the urethra. This cuff is connected to a small pump which is placed in the scrotum and a reservoir which is placed through a small inguinal incision.
To pass urine,Patient presses a small button on the pump placed in the scrotum.The cuff of urethra opens and patients can pass urine in about 45 seconds. The cuff reinflates again in few seconds and patient stops leaking urine.
We have demonstrated and performed this surgery in multiple places around India and also in Bahamas.

Penile Prosthesis:
Patients have problems getting erections, this can be due to natural cause or after pelvic fracture urethral distraction defects.
It’s possible to have a penile prosthesis and get potent again.
We have multiple prosthesis available from different companies. However, there is a “Cafeteria” approach and the patients needs to choose the device he wants.
Indigenously we have the 2 Piece Shahs penile prosthsises. This is a small surgery involving incision at base of penis.2 cylinders are inserted in the penis. The patients can bend the penis and hide the erection in the routine day to day activities.
3-piece penile prosthesis involves an additional button which is placed in the scrotum and a reservoir.
The patients needs to press the button in scrotum, which actually is a pump. The pump helps water stored in the reservoir go in the penile cylinders and there is an erection. After the activity, patient can press the pump again to let the water in cylinder go back to reservoir. This prosthesis is most close to an natural act.



